

Clinical Benefits of the
Printed Try-In
- Comprehensive Pre-Final Verification: Tests passivity, equilibration, aesthetics, tissue adaptation, and speech in a single appointment before zirconia commitment
- Sectioning and Re-luting Capability: Can be divided and reassembled intraorally if passivity issues arise during one-screw Sheffield testing
- Enhanced Patient Visualization: Tooth-colored resin with optional pink gingiva allows realistic aesthetic evaluation and patient approval
- Modification Flexibility: Adjustable with additive composite and reductive contouring to perfect contours and aesthetics
- Speech and Phonetic Testing: Enables comprehensive phonetic evaluation using established test phrases before final fabrication
- Tissue Adaptation Verification: Confirms ideal tissue contact and pressure distribution, preventing final restoration complications
- Quality Control Assurance: Eliminates potential delivery problems by resolving all fit and function issues at the prototype stage
- Multiple Creation Pathways: Can be fabricated from iJIG records, RAPID appliance, or traditional screw-down setups for workflow flexibility
- Documentation and Communication: Provides a physical reference for laboratory communication and a photographic record of required changes

















| Workflow Steps | Instructions | Images |
|---|---|---|
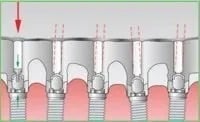
| Step 1 | One-Screw (Sheffield) Test Seat the Printed Try-In placing one screw in the distal most implant on one side and ensure a passive, no-rock seat. Repeat on the other side. If there is rocking, remove a cylinder from the Printed Try-In and pick-up, or section the temp and lute, like a verification jig, until all sections are passive and there is no rock. If no rock is detected, go to next step. |
 |
| Step 2 | Capture x-rays to ensure temp cylinders and abutments are engaged and fully seated. |  |
| Step 3 | Equilibrate and adjust thoroughly. Adjust until the bite and VDO are exact. Adjust for esthetic and functional satisfaction. |  |
| Step 4 | If it is a double arch patient, seat both appliances for the bite. |  |
| Step 5 | Verify that the tissue adaptation is ideal. If not, either remove the prosthesis and digitally scan the tissue, or add some tray adhesive to the intaglio of the prosthesis and take a reline impression using medium body PVS. |  |
| Step 6 | Check for proper lip support and phonetics. To understand how to diagnose and correct phonetic issues refer to ROE’s Full Arch Case Speech Complications for the patient test phrases and how to mitigate identified speech complications. |
 |
| Step 7 | Photograph full-face, full-smile clearly showing what needs changed esthetically. Include opposing model. |  |
| Step 8 | Send all records to ROE Dental Laboratory. Submit your records directly into your patient case via the ROE online portal Next, ROE will fabricate the final prosthesis and send it back to you. |
 |
Frequently Asked Questions
Have question? We are here to help
No results found.